designer, researcher, educator, activist
PHL DESIGN LAB: social sector design
LEARNING SESSION: workshop design and facilitation
BORDER STORIES: design innovation and citizenship
DEGREE SHOW: exhibition design
NHS INFORM FOOD: design research
GLASGOW AS SANCTUARY: activist design
SHIFTING RHYTHMS: community development
NGP VAN: ux/ui design and development
DOULA DESIGN: curriculum design
SEXUAL HEALTH VENDING MACHINE: feminist design
PHL DESIGN LAB FELLOW
OCTOBER 2018-DECEMBER 2018
This project is still in progress, with the hope of completion by March 2019. As such, all work is still in draft form.
how might we redesign the Office of Homelessness prevention, diversion, and intake services?
CONTEXT
the OHS prevention, diversion, and intake services
The PHL Participatory Design Lab, based in the City of Philadelphia, was funded through a generous grant by the Knight Foundation. Beginning in November 2017, the team partnered with the Office of Homeless Services to use service design methods to think through their prevention, diversion, and intake services.
Philadelphia has the highest poverty rate of the nation’s 10 largest cities. This deep poverty, along with a lack of affordable housing, has led to a large homelessness population in the city. The Office of Homeless Services is on the front-lines of preventing at-risk populations from experiencing homelessness, diverting those experiencing homelessness from emergency housing, and providing intake services for those eligible for emergency housing placement. The prevention, diversion, and intake teams manage two access points across the city and those locations were the main focus of this project.
Throughout the course of this project, we co-designed the answer to “What does person-centered and trauma-informed service delivery look like in practice for participants who access and staff who deliver the City of Philadelphia’s prevention, diversion, and intake service?”
A TRAUMA-INFORMED SERVICE EXPERIENCE
providing digestable recommendations to partners
I joined the team in October 2018, after much of the research phase was complete. I focused on translating insights gathered into recommendations for the service experience. Through engagements, the team found that one of the major components of the service was to provide a trauma-informed experience for participants and staff. This meant supporting staff to realize trauma exists in the system, be able to recognize when trauma was present, and respond to that trauma in a way that resists retraumatization. If done successfully, this would lead to collective wellbeing, meaning that all were left better off after interacting with the service experience.
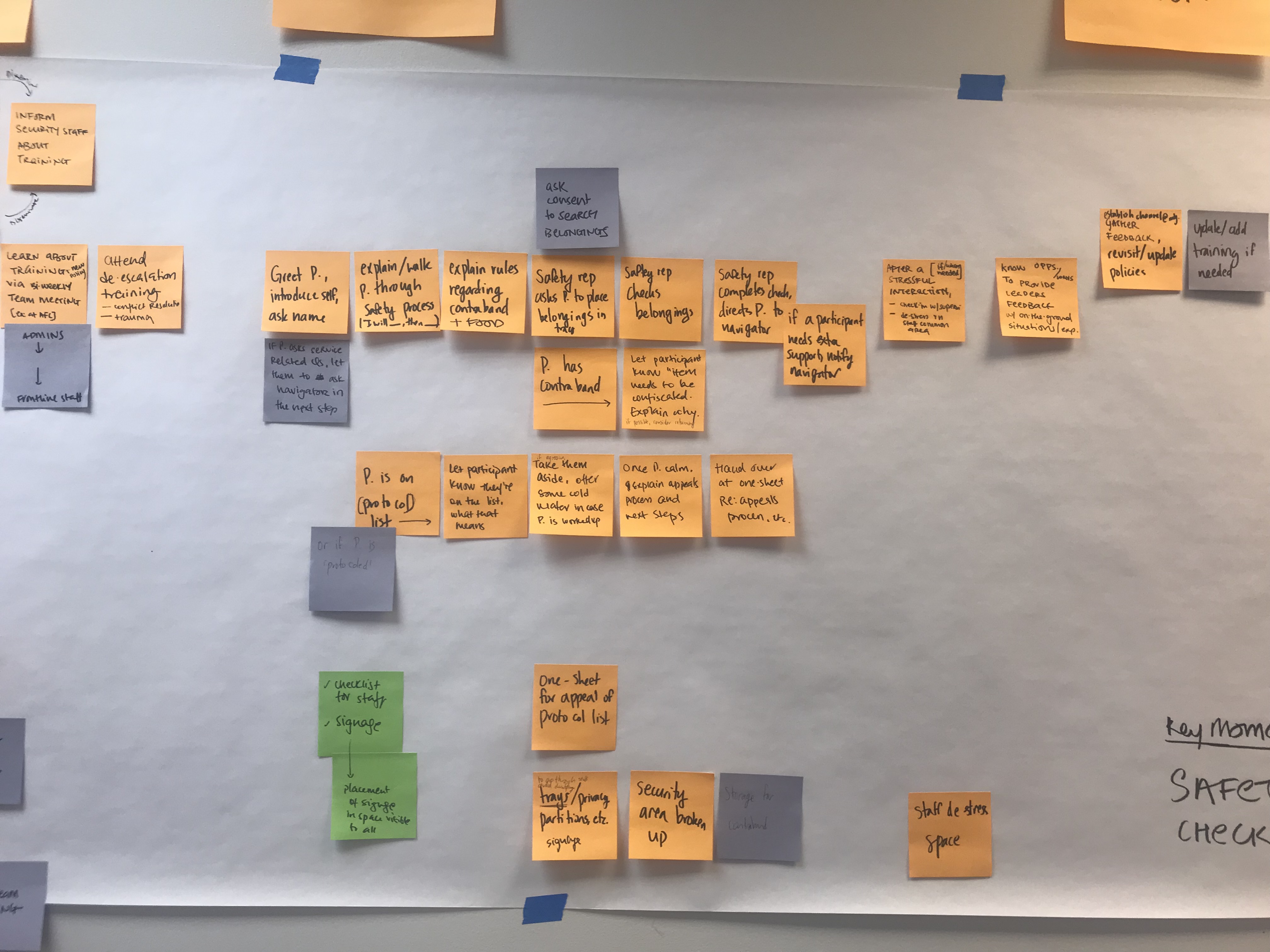
In order to understand how that could be done successfully, we worked to create a set of recommendations around the people, process, space, and information for the prevention, diversion, and intake service experience. In the end, these were brought together through a holistic service journey that mapped these recommendations to key moments within the service experience, providing information about how each concrete moment could be more trauma-informed for both participants and staff.